
“Please Don’t Call It Gross”: Living With Body-Focused Repetitive Behaviors in Silence

- Authors

- Name
- Author: HealthUnspoken Editorial Team
- Published on
- Last updated:
- Country
- Country
- 🌍Country: Global
There are things people live with for years that never make it into conversation—not because they’re rare, but because one reaction can shut the door forever. A raised eyebrow. A half-smile. That tiny moment when you realize the other person is about to label you.
This is a de-identified story about Body-Focused Repetitive Behaviors (BFRBs)—repetitive actions like nail biting, skin picking, or cheek chewing. It’s written in a human voice because that’s how it’s lived: not as a “fun fact,” not as a quirky trait, but as something complicated, exhausting, and often invisible.
A quiet pattern that starts early
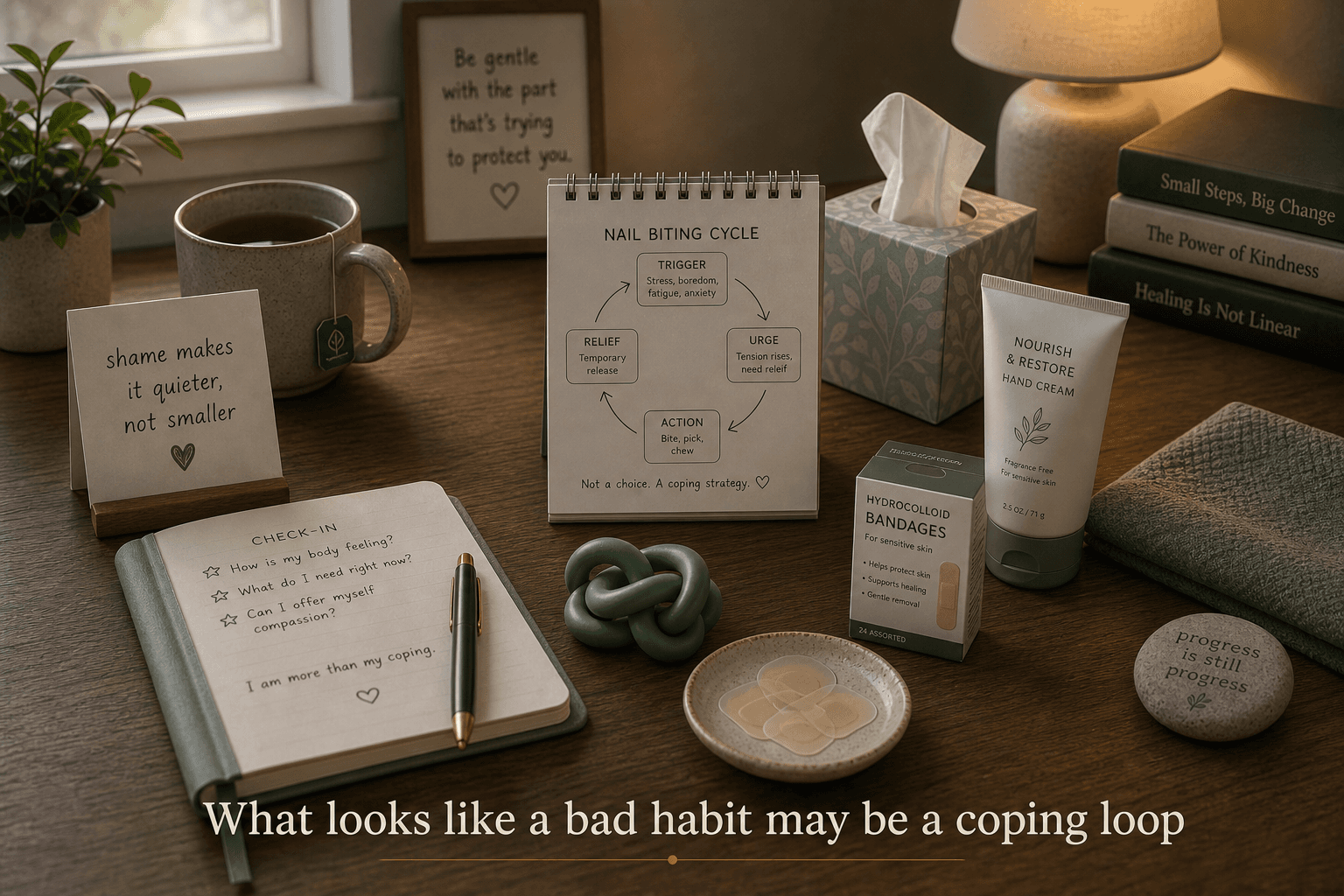
For one person, it began in childhood the way many habits do—small, easy to miss. Nails bitten down. Skin around fingers picked until it looked raw. It wasn’t a “phase.” It was a loop. And because it didn’t come with a dramatic announcement, it lived in the background.
Parents noticed the surface signs sometimes. But the deeper part—the urge, the trance, the after—was harder to see.
And that’s the part most people don’t understand:
these behaviors aren’t always a decision. Sometimes they feel like a reflex. Sometimes they happen while your mind is somewhere else.
“If you call it disgusting, I won’t tell you anything”
There’s a line that stuck with me while reading this person’s experience:
People don’t hide because they don’t know.
They hide because they do know.
They know it can look odd.
They know it can be unhygienic.
They know it’s not something you casually bring up at dinner.
So when someone—especially someone close—reacts with disgust, even subtly, the message lands hard:
“Don’t talk about this again.”
That one moment can turn a manageable struggle into a private life sentence.
And that’s why “just stop” doesn’t work.
Not because the person hasn’t tried.
But because the behavior isn’t only a habit—it’s often tied to stress, focus, overwhelm, or emotional overload.
The invisible fuel: anxiety, neurodivergence, and difficulty naming emotions
This person had diagnoses like ADHD and anxiety, and also described signs of neurodivergence and difficulty identifying and describing emotions (often called alexithymia).
That combination matters because it can create a perfect storm:
- you feel uncomfortable or overloaded,
- you can’t easily name what you’re feeling,
- and your brain reaches for something that creates short-term relief.
Sometimes that relief comes from movement. Sometimes from pressure. Sometimes from repetitive behaviors that feel “automatic.”
Not everyone with BFRBs has the same background, and not everyone has the same pattern. But it’s common for these issues to overlap.
When it starts to cost you—time, skin, confidence
One of the hardest parts in this story is not the behavior itself.
It’s the hours.
This person described zoning out and picking or chewing for long stretches without realizing. The body gets tired. Joints ache. Posture collapses. You come back to yourself and feel shocked by how much time disappeared.
Then comes the second punch: checking the mirror or touching your skin and feeling the damage.
That’s often where shame gets louder.
And shame is a powerful trap. Because shame increases stress. And stress increases urges. And the loop deepens.
What the comment patterns suggested
I pulled bounded MySQL samples before updating this article. The results were smaller and noisier than some of the other topics, but the recurring themes were still useful.
The clearest patterns were:
- people feeling embarrassed to admit they were picking, chewing, or pulling at all
- mirror time making the urge worse once someone noticed an imperfection or rough spot
- burnout, racing thoughts, and middle-of-the-night stress making repetitive behaviors more intense
- people asking for help after years of hiding it because family reactions had already taught them to stay quiet
- frustration that broad advice like "just stop" or even treatment alone did not automatically change the loop
That matches the lived pattern in this story.
These behaviors often sit at the intersection of stress, sensory discomfort, shame, and automatic repetition. If you only address the visible damage, you miss the conditions that keep restarting it.
“I’m not lazy. I’m stuck.”
The story also touched something many people relate to: the way mental health can look like laziness from the outside.
When you’re overwhelmed, you might miss assignments. Avoid tasks. Stay in bed longer than you want to. Not because you don’t care—because your brain and body feel jammed.
Sometimes the behaviors spike exactly when things matter most: exams, deadlines, major transitions. The pressure doesn’t push you forward. It pushes you into coping.
And that’s why judgment doesn’t help.
It only adds weight to an already overloaded system.
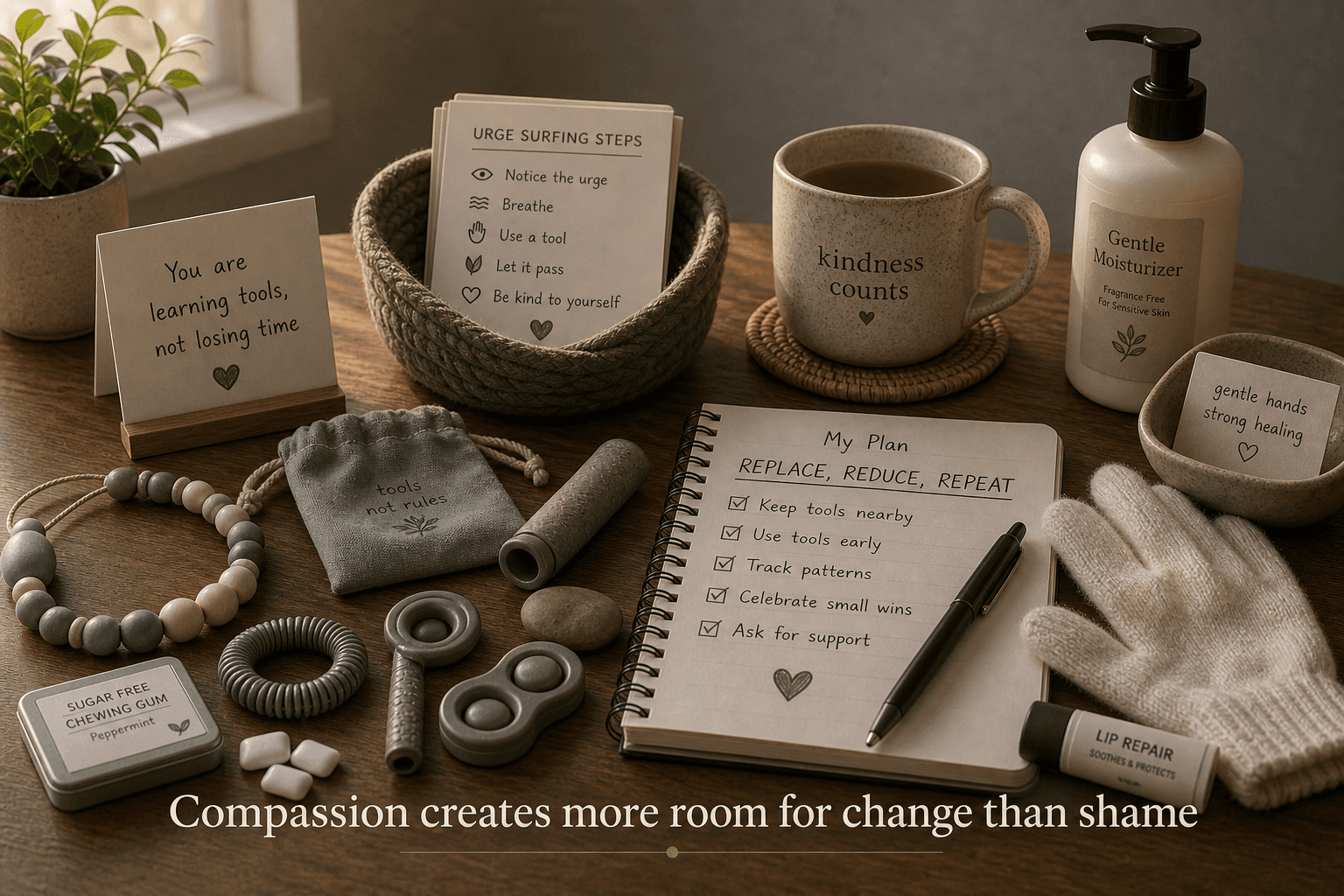
What helps more than “stop”: replace, reduce, repeat
There’s a practical insight in this person’s journey that deserves more attention:
Harm reduction beats perfection.
Instead of expecting instant change, it helped to redirect the behavior toward something safer.
For example:
- a chewable necklace,
- gum,
- a fidget,
- moisturizer, bandages, or smoother skin barriers,
- a routine that gently interrupts the “zoning out” pattern.
It wasn’t magical. It didn’t erase the urge overnight.
But it created a bridge: from “I can’t stop” to “I can shift.”
That’s a big difference.
Because when you feel a little control, the shame eases.
And when shame eases, the urge often becomes less intense.
The complicated part: wanting help, fearing the reaction
This person described being afraid to seek professional support—not because they didn’t want it, but because they feared judgment.
That fear makes sense. People do get judged. Even by well-meaning family members. Even by people who should know better.
And the scary part is: one facial expression can do more damage than a lecture.
If you’re someone trying to support a person with BFRBs, here’s the simplest rule:
Don’t lead with disgust.
Lead with curiosity and respect.
Even a calm sentence like:
- “Thanks for telling me.”
- “That sounds exhausting.”
- “What helps even a little?” can change the entire conversation.
A note on safety and urgency (without labels)
The person writing this story questioned whether their situation would ever be treated seriously unless it looked like an emergency.
That’s a painful reality for many people: support often arrives late, after things escalate.
BFRBs can range from mild to severe. When they cause ongoing injury, distress, or major life disruption, they deserve attention. Not dismissal.
If someone reading this feels stuck, it’s okay to start small:
- talk to a trusted clinician,
- look for a therapist familiar with BFRBs,
- notice specific triggers like mirrors, fatigue, rough skin, or long idle stretches,
- explore evidence-based approaches like Habit Reversal Training (HRT) or broader CBT-based support.
You don’t need to “prove” suffering to deserve help.
The unexpected upside: healing changes the mind too
One of the most hopeful parts of this story is also the simplest:
When the person let their body heal—even for a while—they felt better.
More confident.
More positive.
More “themselves.”
That doesn’t mean healing is easy. It means it’s worth it.
Sometimes the body is the doorway back to the mind.
Not through punishment—but through care.
If you’re trying to help someone like this
Here’s what this story teaches, in plain terms:
- Don’t shame them.
- Don’t treat it like a gross secret.
- Don’t demand instant stopping.
- Help them replace the behavior, slowly.
- Praise progress that looks small.
- Respect boundaries if they don’t want details.
- Keep the conversation open so they don’t have to carry it alone.
Because the biggest risk isn’t always the behavior itself.
The biggest risk is that someone feels so judged they never ask for help again.
Final thoughts
Some problems don’t announce themselves.
They hide behind jokes, silence, and “I’m fine.”
If this story felt familiar, you’re not alone—and you’re not broken.
You’re a human being with a coping pattern that got too heavy to carry.
And you deserve support that doesn’t make you feel less human.
References
- NHS: Skin picking disorder
- TLC Foundation for Body-Focused Repetitive Behaviors: What are BFRBs?
- MedlinePlus: Nail biting
Related HealthUnspoken Reading
Disclaimer: This article is for educational purposes only and is not medical advice. Body-focused repetitive behaviors can overlap with anxiety, ADHD, OCD-related conditions, trauma, or sensory regulation problems. If picking, biting, chewing, or hair pulling is causing skin damage, infection, bleeding, major distress, or disruption to daily life, seek help from a qualified clinician or mental health professional.
Short version for YouTube Short / FB / WhatsApp
Option A (voiceover, ~20–25 sec)
Some habits aren’t “gross”—they’re coping.
Body-focused repetitive behaviors like skin picking or cheek chewing can happen automatically, especially with anxiety or ADHD.
Shame doesn’t stop it. It just makes people hide it.
What helps is compassion and small replacements—like gum or a chew tool—one step at a time.
Option B (caption-style, ~2–3 lines)
If someone opens up about BFRBs, don’t react with disgust.
Shame makes it worse.
Compassion + small replacements can work better than “just stop.”
Option C (WhatsApp status, 1 line)
Some “bad habits” are actually hidden coping—compassion helps more than judgment.
Related Reading
Continue reading after “Please Don’t Call It Gross”: Living With Body-Focused Repetitive Behaviors in Silence
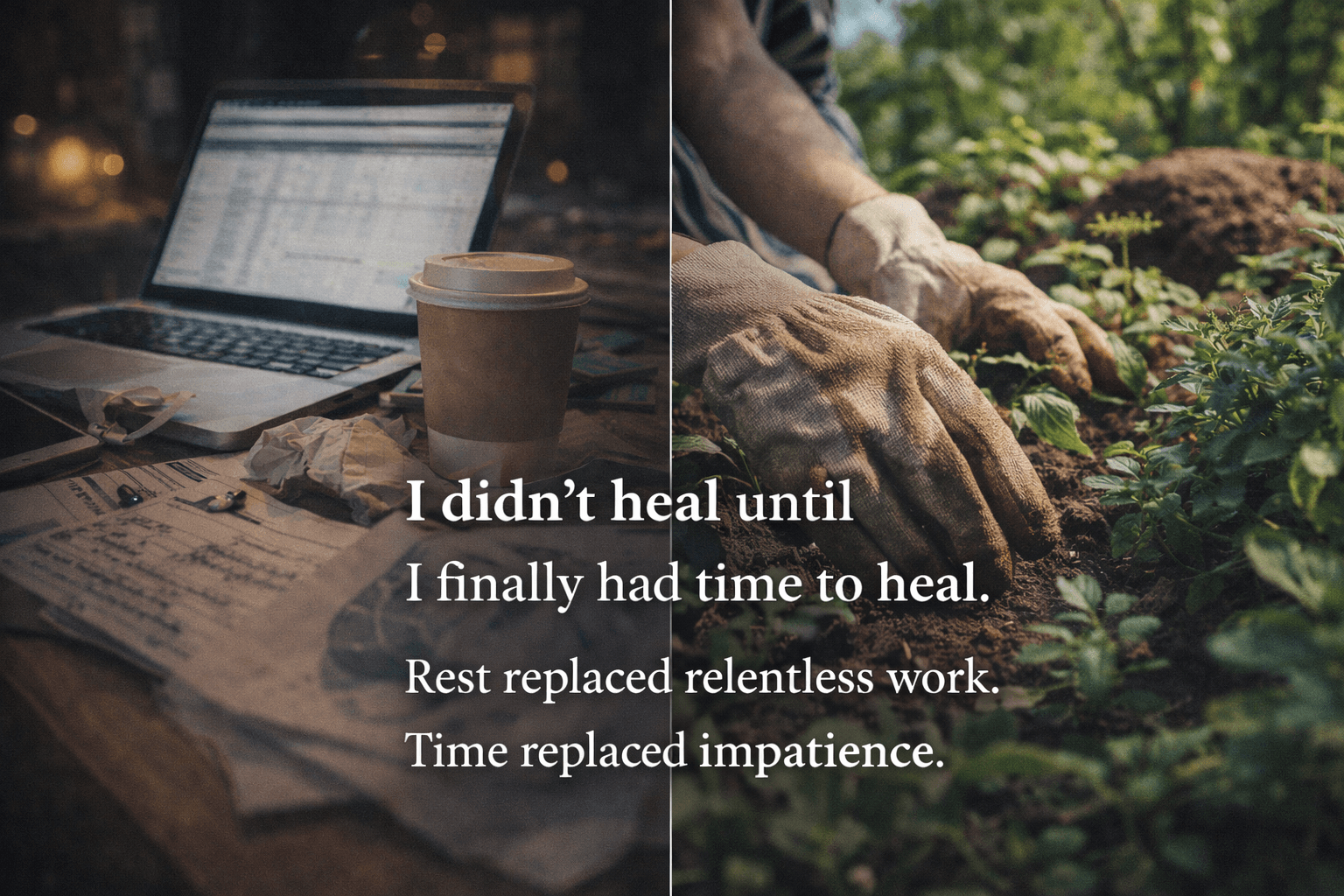
I Didnt Heal Until I Finally Had Time to Heal
A de-identified personal story about chronic pain, constant work urgency, burnout, nervous-system exhaustion, and the slower kind of recovery that only started once rest became real instead of theoretical.

Living With a Dry Mouth, Burning Pain, and No Easy Answers
A lived experience of chronic dry mouth, burning pain, medication side effects, dental damage, broken sleep, and the slow search for safer support.
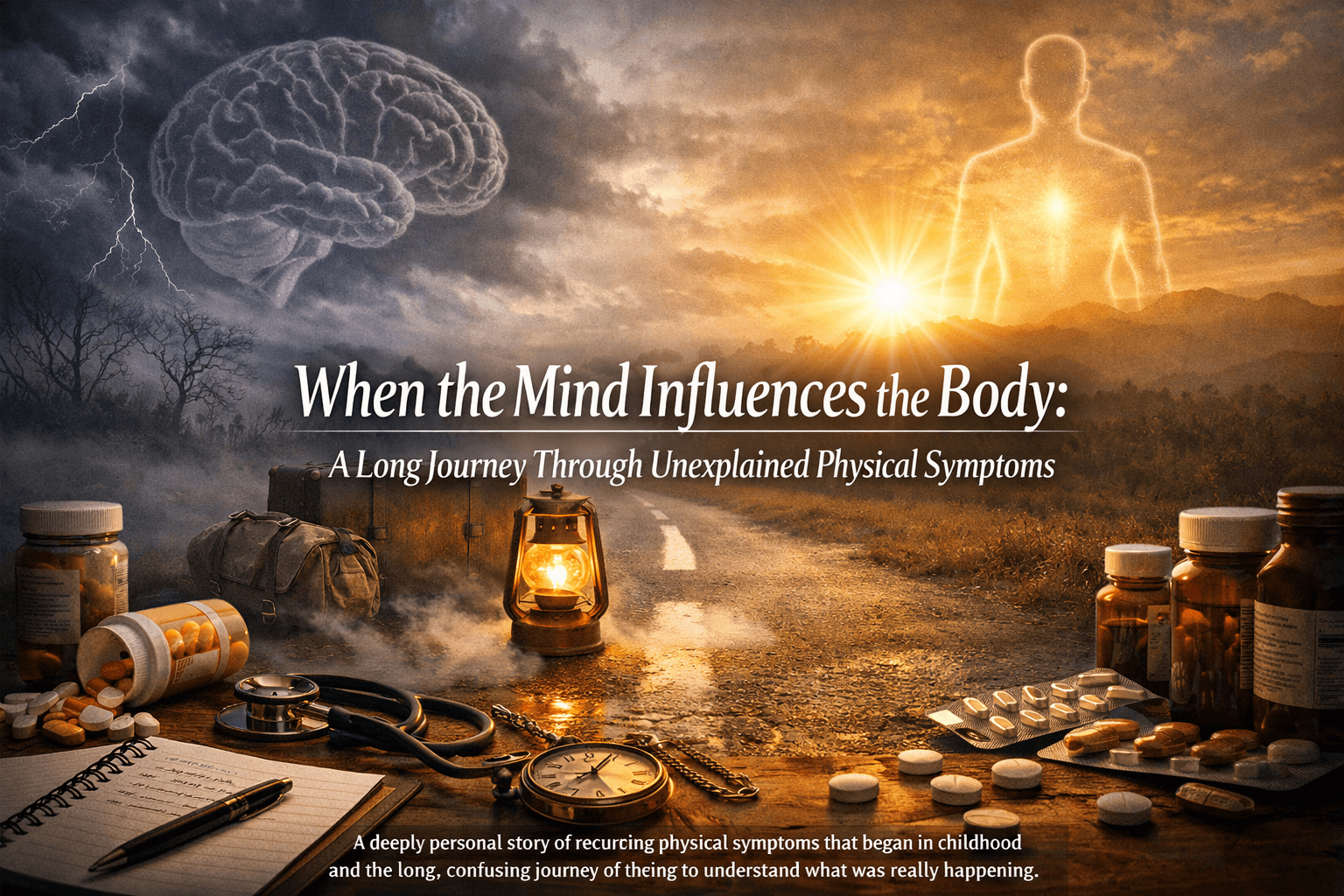
When the Mind Influences the Body: A Long Journey Through Unexplained Physical Symptoms
A deeply personal story of recurring physical symptoms that began in childhood and the long, confusing journey of trying to understand what was really happening.
Share on WhatsApp
2–3 line summary is copied. Tap to open WhatsApp and share.
 Tip: You can edit the text after it opens in WhatsApp.
Tip: You can edit the text after it opens in WhatsApp.Editorial Note
This article is prepared by the HealthUnspoken Editorial Team. Our articles may combine first-person submissions, public health education references, and commonly discussed experiences, then are edited for clarity and context.
The goal is reader awareness and education. This content is not a diagnosis or a treatment plan.
⚕️ Medical Disclaimer
The information provided in this article is for **educational and informational purposes only**. It should not be considered medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider regarding any medical condition or treatment decisions.
🧾 Sources
HealthUnspoken articles may include first-person stories, editorial summaries of broadly discussed experiences, and public health education references. They are reviewed by the editorial team for clarity and educational context.
Reader Experiences Shared
Curated anonymized snippets from public health discussions, edited for readability.
I kept thinking bfrb silence compassion would settle on its own, but what helped most was tracking patterns and asking clearer questions in appointments.
The hardest part for me was uncertainty around bfrb silence compassion. Once I stopped changing everything at once, I could finally see what was helping.
I used to delay care because I was embarrassed about bfrb silence compassion. Earlier conversations would have saved me a lot of stress.
A second opinion around bfrb silence compassion changed my decisions completely. The issue was still real, but the plan felt calmer and more practical.
For me, progress with bfrb silence compassion came from boring consistency, not one dramatic fix. That mindset reduced panic a lot.
I learned to separate fear from facts with bfrb silence compassion. Writing down symptoms before visits made discussions more useful.